

Latest Story
-

Trust the science
Doug Hilton | April 16, 2024We need science to tackle the big challenges of today, so we must defend it from attack. While Australia isn’t as polarised as the US about scientific trust and issues, we can’t afford to be complacent.
-
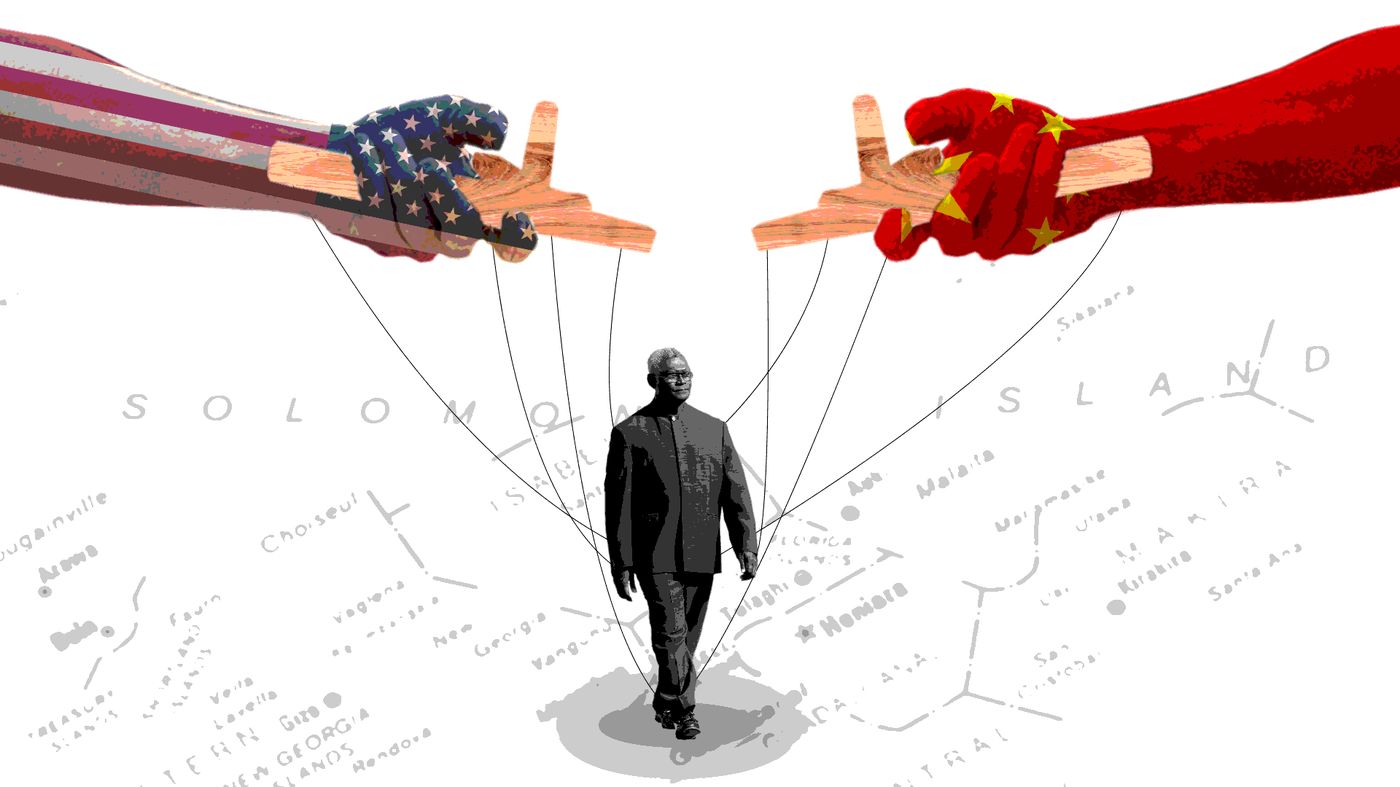
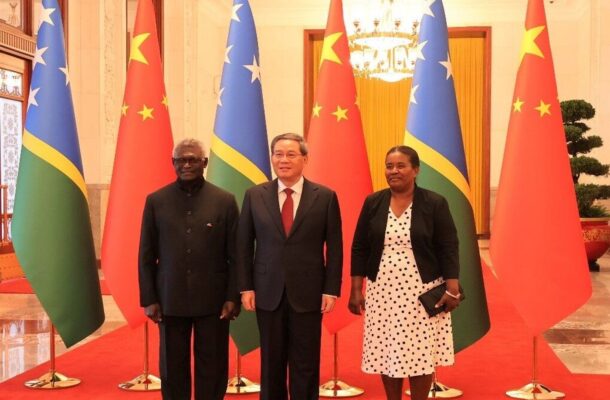
Understanding the Solomons elections
Priestley Habru | April 16, 2024Prime Minister Manasseh Sogavare is looking to retain power on April 17 in what could prove a vital day for the geo-political future not just of the Solomon Islands, but the whole Pacific.
-

Innovate and grow
Open Forum | April 16, 2024Australia’s national science agency, CSIRO, is inviting small to medium enterprises (SMEs) working on advanced manufacturing solutions to apply for a self-paced, 10-week, online program that can help them turn an idea into an R&D opportunity.
-

A farewell to arms?
John Tilemann | April 15, 2024With war raging in Ukraine and the Middle East it’s difficult to remember that the international system has accepted growing constraints on interstate use of force in most circumstances.
-

Mapping global cybercrime
Open Forum | April 15, 2024Three years of intensive research by an international team of researchers has informed the first ‘World Cybercrime Index’ which ranks Russia as the major threat to global cyber security.
-

Science is the key to our manufacturing future
Open Forum | April 15, 2024The Australian Academy of Science has welcomed the Prime Minister’s intention to legislate a “Future Made in Australia Act” to boost technologically advanced manufacturing in this country.
-
Reforming public service leadership
Odette Meli | April 14, 2024Australia’s public service needs a more robust system for decision-making and policy planning to navigate increasing complexities and become more resilient to change.
-

Growing apart
Open Forum | April 14, 2024Cultural values may have become more different globally, but more similar regionally, over the past 40 years, according to US researchers who analysed the data from the ‘World Values Survey’, which includes more than 400,000 people from 76 countries.
-

The last election?
Anouk Ride | April 14, 2024Solomon Islanders are set to vote on 17 April in an election that has significance within and beyond the country’s borders due to Prime Minister Manasseh Sogavare’s increasingly authoritarian stance and backing from China.
-
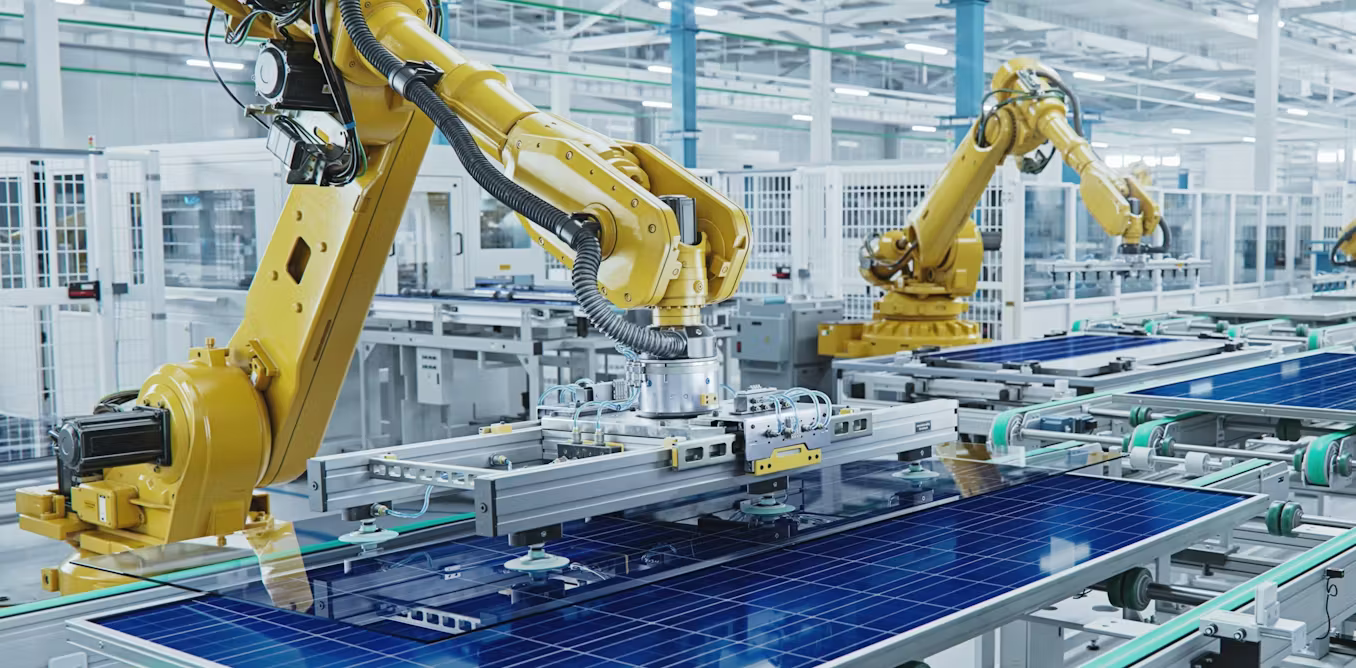
Fashioning the future
Naoise McDonagh | April 13, 2024Whatever risks the Albanese government may face in encouraging cutting-edge manufacturing, it has avoided the much greater risk of doing nothing at all in the face of historic global economic change.
-

Centigrade cartography
Open Forum | April 13, 2024Advocacy groups have welcomed the release of the Federal Government’s announcement of a heat mapping tool to assist affected communities deal with the worst of extreme heat.
-

Into the shimmering world
Ian Maxwell | April 13, 2024Angus Cerini’s play Into the Shimmering World, now playing in Sydney, is an unforgiving meditation on what it is to be good and what takes to live a good life.






